Our Evidence
12+ years of clinical evidence (within PPH applications) vs standard of care demonstrating a Safe and Clinically effective technology.

More studies below

12+ years of clinical evidence (within PPH applications) vs standard of care demonstrating a Safe and Clinically effective technology.
More studies below
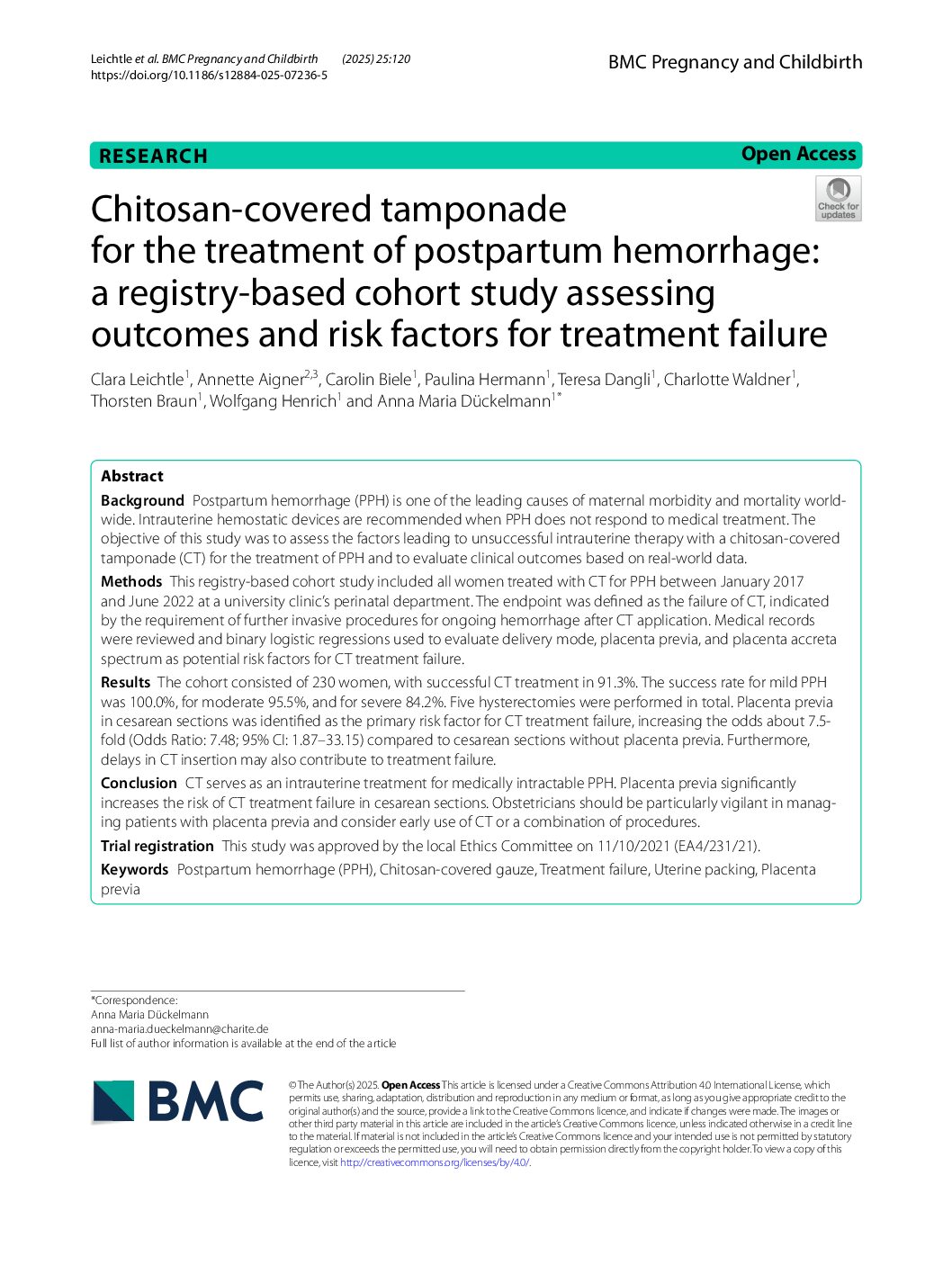
BMC Pregnancy Childbirth. 2025 Feb 5;25(1):120. doi: 10.1186/s12884-025-07236-5.
Background: Postpartum hemorrhage (PPH) is one of the leading causes of maternal morbidity and mortality worldwide. Intrauterine hemostatic devices are recommended when PPH does not respond to medical treatment. The objective of this study was to assess the factors leading to unsuccessful intrauterine therapy with a chitosan-covered tamponade (CT) for the treatment of PPH and to evaluate clinical outcomes based on real-world data.
Methods: This registry-based cohort study included all women treated with CT for PPH between January 2017 and June 2022 at a university clinic's perinatal department. The endpoint was defined as the failure of CT, indicated by the requirement of further invasive procedures for ongoing hemorrhage after CT application. Medical records were reviewed and binary logistic regressions used to evaluate delivery mode, placenta previa, and placenta accreta spectrum as potential risk factors for CT treatment failure.
Results: The cohort consisted of 230 women, with successful CT treatment in 91.3%. The success rate for mild PPH was 100.0%, for moderate 95.5%, and for severe 84.2%. Five hysterectomies were performed in total. Placenta previa in cesarean sections was identified as the primary risk factor for CT treatment failure, increasing the odds about 7.5-fold (Odds Ratio: 7.48; 95% CI: 1.87-33.15) compared to cesarean sections without placenta previa. Furthermore, delays in CT insertion may also contribute to treatment failure.
Conclusion: CT serves as an intrauterine treatment for medically intractable PPH. Placenta previa significantly increases the risk of CT treatment failure in cesarean sections. Obstetricians should be particularly vigilant in managing patients with placenta previa and consider early use of CT or a combination of procedures.
Trial registration: This study was approved by the local Ethics Committee on 11/10/2021 (EA4/231/21).

Department of Obstetrics, Charité – University Hospital Berlin, Berlin, Germany - 23rd May 2024
Anna M. Dückelmann, Paulina Hermann, Carolin Biele, Clara Leichtle, Charlotte Waldner,
Thorsten Braun and Wolfgang Henrich.
Objective: This retrospective follow-up study analyzes the effect of intrauterine postpartum hemorrhage (PPH) therapy on menstrual, reproductive, and mental health outcomes.
Methods: All women who delivered at a university hospital between 2016 and 2021 with PPH and who needed intrauterine therapy were included. A questionnaire on well-being, menses, fertility, and reproductive outcomes was mailed to the patients. Those who did not reply were surveyed by telephone.
Results: A total of 214 women treated with chitosan-covered gauze (group A) and 46 women treated with a balloon tamponade (group B) were recruited, and their short-term courses were analyzed. For long-term follow-up, 71 women of group A (33%) and 21 women of group B (46%) could be reached. A total of 89% of group A and 95% of group B had regular menstrual bleeding in the most recent 12months; 27% (group A) and 29% (group B) were trying to conceive again, and all of them did so successfully. There were 12 deliveries, 3 ongoing pregnancies, 3 miscarriages, and 2 terminations of pregnancies (TOP) in group A and 4 deliveries, 1 miscarriage, and 2 TOPs in group B. More than half of our study participants was sorted into grade II or III of the Impact of Events Scale, indicating they experienced clinical impacts in the form of psychological sequelae. One-quarter of patients had symptoms of post-traumatic stress disorder.
Conclusion: Chitosan gauze as well as balloon tamponade appear to have few adverse effects on subsequent menstrual and reproductive function. Women after PPH are at increased risk of long-term adverse psychological outcomes.
https://www.tandfonline.com/doi/pdf/10.1080/14767058.2024.2354382
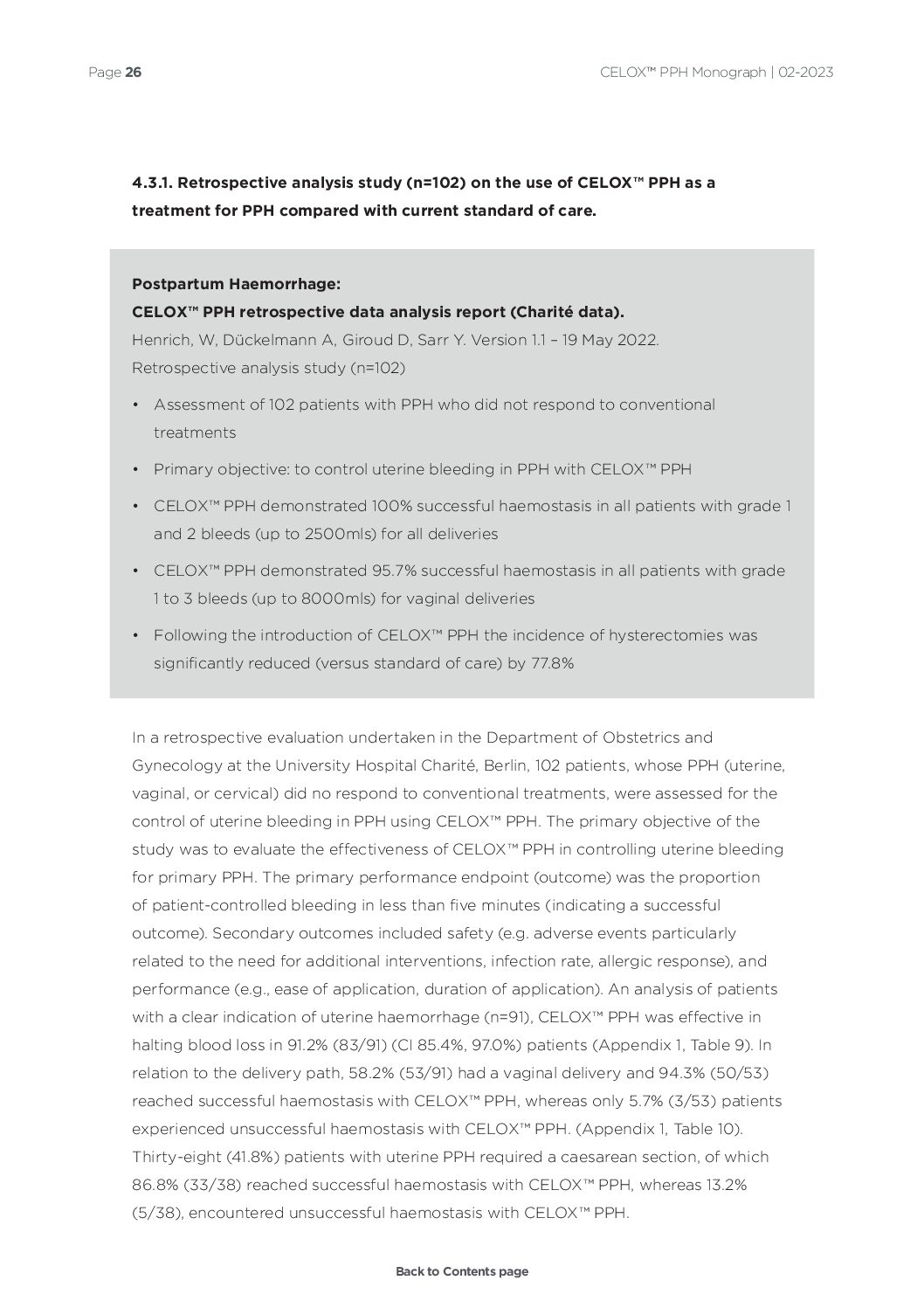
Postpartum Haemorrhage:
CELOX™ PPH Gauze retrospective data analysis report (Charité data).
Henrich, W, Dückelmann A, Giroud D, Sarr Y. Version 1.1 – 19 May 2022.
Retrospective analysis study (n=102)
Uterine packing with CELOX™ PPH compared to balloon tamponade for managing postpartum haemorrhage.
Dueckelmann AM, Hinkson L, Nonnenmacher A, Siedentopf JP, Schoenborn I, Weizsaecker K, Kaufner L, Henrich W, Braun T. Eur J Obstet Gynecol Reprod Biol. 2019; 240:151-155.
Retrospective cohort study (n=78)
Roberto Velasco Sordo 1, Humberto López Maldonado 1, Daniel A Ramirez Flores 1, Eduardo Ibarrola Buen Abad 1, Pablo Vilchis Nava 1
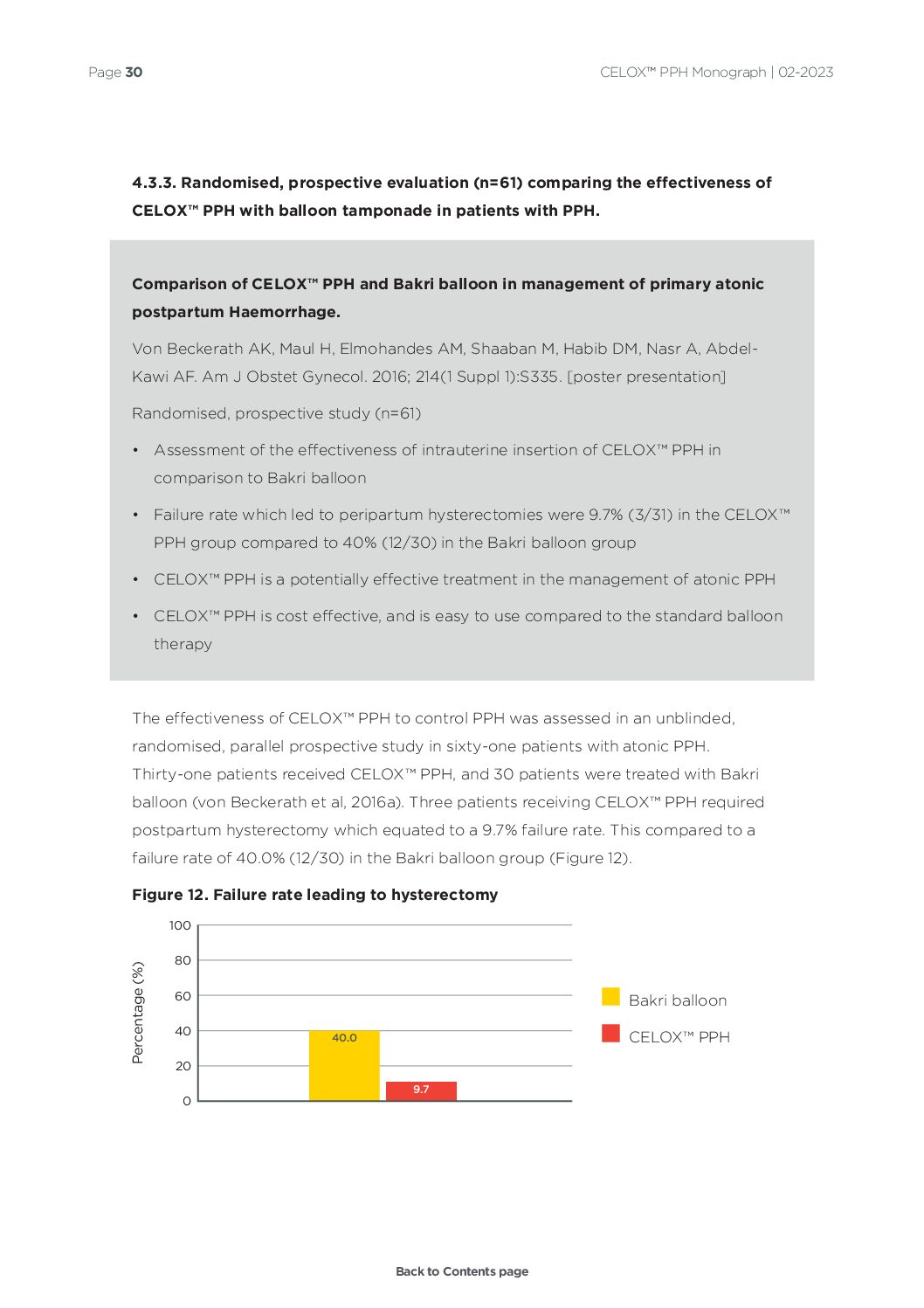
Comparison of CELOX™ PPH and Bakri balloon in management of primary atonic postpartum Haemorrhage.
Von Beckerath AK, Maul H, Elmohandes AM, Shaaban M, Habib DM, Nasr A, Abdel-Kawi AF. Am J Obstet Gynecol. 2016; 214(1 Suppl 1):S335. [poster presentation]
Randomised, prospective study (n=61)
Does the use of CELOX™ PPH for postpartum haemorrhage reduce the need for surgical therapy including hysterectomy? A databased historical cohort study.
Biele C, Radtke L, Kaufner L, Hinkson L, Braun T, Henrich W, Dückelmann AM. J Perinat Med. 2022; 50(8):1078-1086.
Retrospective cohort study (n=666)
Use of CELOX™ PPH in 98 cases of severe postpartum haemorrhage–a multicenter registry analysis.
Von Beckerath AK, Maul H, Gebauer G, Abdel-Kawi AF, Rolf N, Saade G, Bader W, Kusnierczak D, Berger R, Kienast C, Kienemund J, Schmid B. Am J Obstet Gynecol. 2016; 214(1 Suppl 1):S269. [poster presentation]
Multicentre registry analysis study (n=98)

Uterine packing with CELOX™ PPH for control of postpartum Haemorrhage (PPH).
Maul H, Steinmacher S, Saade G, Gebauer G, Rolf N, Schmid B. Am J Obstet Gynecol. 2015; 212(1 Suppl 1):S358-S359. [poster presentation]
Case study series (n=65)
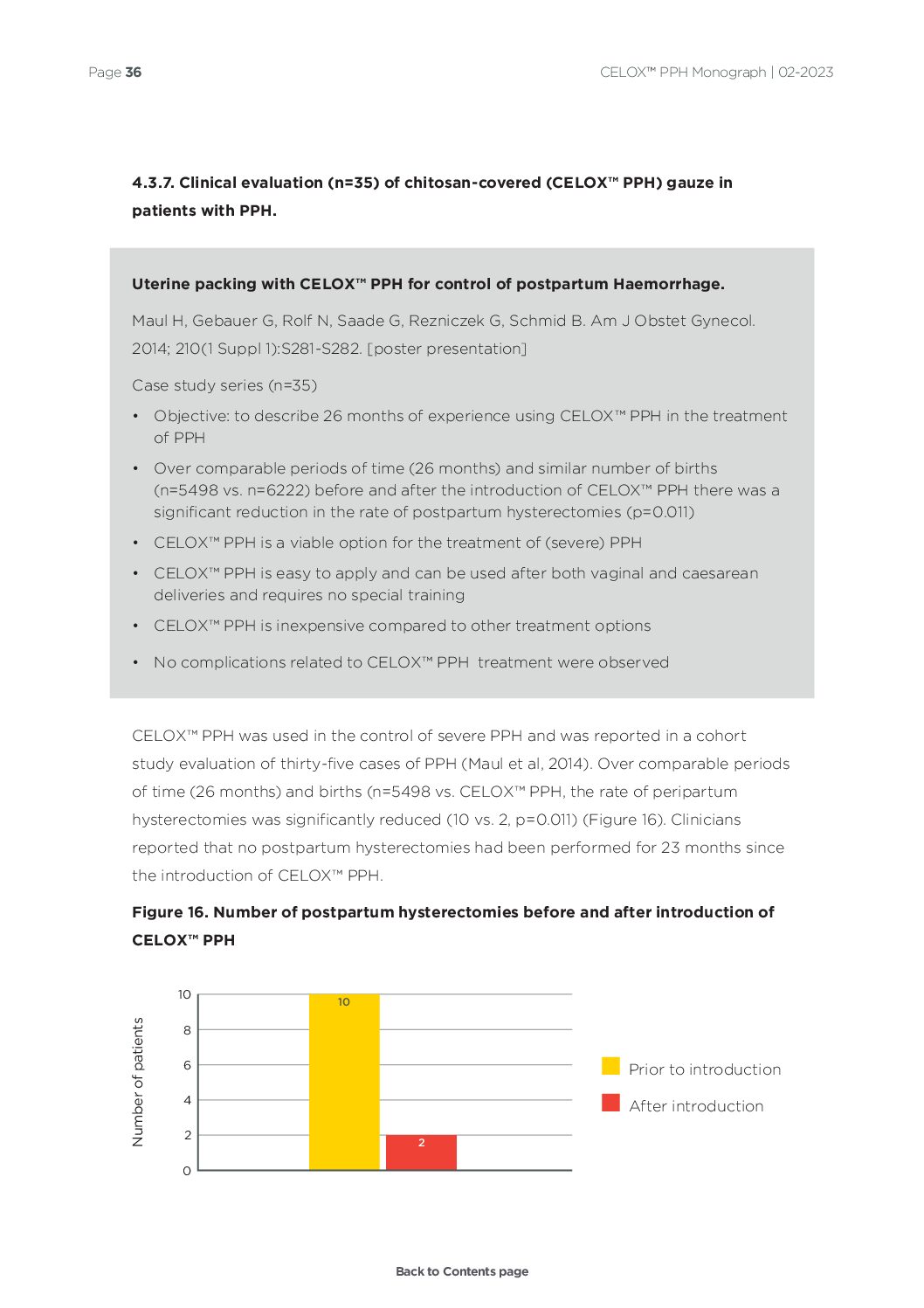
Uterine packing with CELOX™ PPH for control of postpartum Haemorrhage.
Maul H, Gebauer G, Rolf N, Saade G, Rezniczek G, Schmid B. Am J Obstet Gynecol. 2014; 210(1 Suppl 1):S281-S282. [poster presentation]
Case study series (n=35)
Uterine packing with CELOX™ PPH for control of postpartum Haemorrhage.
Schmid BC, Rezniczek GA, Rolf N, Saade G, Gebauer G, Maul H.. Am J Obstet Gynecol. 2013; 209(3):225.e1-225.e5.
Case study series (n=19)

Uses of CELOX™ PPH for treating different forms of serious obstetrics haemorrhages.
Carles G, Dabiri C, Mchirgui A, Saoudi EO, Hcini N, Pouget K, Seve B, de Matteis B. J Gynecol Obstet Hum Reprod. 2017; 46(9):693-695.
Case study series (n=4)
Application of CELOX™ PPH in combination with intrauterine balloon tamponade for postpartum Haemorrhage treatment – Case report of a novel "uterine sandwich" approach.
Seidel V, Braun T, Weizsäcker K, Henrich W. Int J Surg Case Rep. 2018; 48:101-103.
Case report (n=1)
Postpartum Haemorrhage: use of CELOX™ PPH.
Schmid BC, Rezniczek GA, Rolf N, Maul H. Am J Obstet Gynecol. 2012; 206(1):e12-e13.
Case report (n=1)

American Journal of Obstetrics & Gynecology - Expert Review
Wolfgang Henrich, MD, PhD; Anna Dückelmann, MD; Thorsten Braun, MD, PhD;
Larry Hinkson, MBBS, MD, MRCOG, FRCOG
Postpartum hemorrhage (PPH) causes substantial maternal mortality and morbidity and is responsible for a quarter of all maternal deaths worldwide.1 Conventional use of uterotonics such as oxytocin, prostaglandins, and medications to support coagulation, such as fibrinogen and tranexamic acid, are helpful but may not be sufficient to arrest life-threatening PPH. Blood transfusions, intrauterine balloon tamponade application, invasive techniques, such as compression sutures, and arterial ligation are advanced steps in the management cascade. In extreme cases, a hysterectomy may be necessary to avoid maternal death.
Medtrade Products Ltd,
Electra House,
Crewe Business Park,
Crewe, Cheshire, England,
CW1 6GL
Tel: +44 (0)1270 500 019
Email: info@celoxpph.com
This website uses Cookies to improve your browsing experience and to help with our marketing. You can read more about removing Cookies here: Cookie Policy
I'm fine with this